Case #1: Too Many Pills
Author: Jami Hickey, MD
Peer Reviewer: Mark Mycyk, MD
A 45 year old female with a past medical history of depression presents to the emergency department after reportedly taking a bottle of pills at home 30 minutes prior to arrival in a suicide attempt. She is alert and oriented on arrival with no complaints. She does not remember the name of the pill, but states that it was prescribed for her depression.
Vitals: T: 98.6, HR: 120, RR: 14, BP: 118/70, O2 Sat: 100% on RA
Shortly after, the patient’s friend arrives at the hospital with an empty bottle of amitriptyline and the patient confirms that this is what she took.
What clinical presentations might you expect to see with this drug?
Initially, the patient may have minimal symptoms. Later, the patient may develop both CNS and cardiac symptoms, including:
-Altered mental status (sedation, seizures, coma)
-Mild to severe anticholinergic symptoms
-Hypotension (both due to the alpha-1 antagonism and direct myocardial depression)
-Severe cardiotoxicity (due to the fast Na channel blockade)
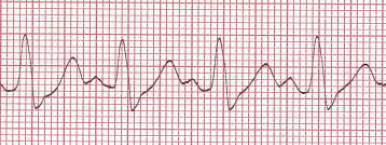
What are the possible ECG findings in this TCA overdose?
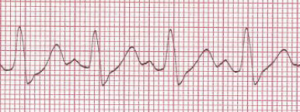
(Courtesy of James Heilman, MD – Wikimedia Commons)
-Sinus tachycardia (most common)
-Right axis deviation with a R wave in aVR
-Prolongation of the PR, QRS, and QTc intervals.
Note: The QTc may be prolonged at therapeutic dosages of TCAs, as well.
Over what time period do patients typically exhibit symptoms of overdose?
-Most fatalities occur within the first few hours of overdose.
-Serious toxicity is almost always seen within 6 hours of overdose. Note: This is the origin of the famous “6 hour” rule for observation in Toxicology.
-ECG abnormalities begin within 6 hours of overdose and resolve over the subsequent 36-48 hours.
What treatments should be considered?
-Consider early intubation if the patient experiences CNS depression or hemodynamic instability.
-Activated Charcoal can also be considered if the ingestion is within 30-60 mins and the patient is asymptomatic and able to protect airway. Gastric lavage not recommended.
-Sodium Bicarbonate boluses are recommended to overcome the sodium channel blockade. Therapy is indicated for refractory hypotension, cardiac conduction abnormalities, or ventricular dysrhythmias.
–Note: This is given as boluses, NOT as a drip.
– Benzodiazepines should be given for seizures and symptomatic management. Phenobarbital is the second line treatment (Note: Phenytoin is more useful for seizures with anatomical foci and is not recommended for TCA-related seizures).
-Intralipid therapy may be considered if the above treatment has been provided and the patient is still deteriorating or not improving. Intralipid works by binding the TCAs, which are highly lipid soluble.
Are TCAs dialyzable?
-Hemodialysis is not effective in enhancing elimination due to the large volume of distribution (Vd), extensive protein binding, and high lipid solubility.
Dialyzable drug criteria:
-Small Vd
-Poor protein binding
-Highly water soluble
-Low molecular weight
Which former “coma cocktail” drug is contraindicated in suspected TCA overdose?
-Physostigmine has been reported to increase the risk of cardiac toxicity (bradycardia and asystole) and seizures.
References:
Harrigan RA, Brady WJ. ECG abnormalities in tricyclic antidepressant ingestion. Am J Emerg Med. 1999 Jul;17(4):387-93.
Liebelt EL, Ulrich A, Francis PD, et al. Serial electrocardiogram changes in acute tricyclic antidepressant overdoses. Crit Care Med. 1997 Oct;25(10):1721-6.
Return to Case List